Otalgia
Flowchart

Red flags requiring urgent ENT referral
Associated facial nerve palsy
Spreading cellulitis
Systemically unwell
Neurological signs
Suspected mastoiditis (red, tender mass behind ear in unwell patient with AOM)
Suspected lateral skull base ostoemyelitis (out-of-proportion ear pain in diabetic/elderly patient)
Assessment and recognition
History
How long have you had ear pain? Does it come and go?
Where is the pain? Does it spread anywhere?
Other otological symptoms (otorrhoea, tinnitus, hearing loss, vertigo, facial weakness).
Upper aerodigestive tract red-flag symptoms (dysphagia, odynophagia, dysphonia, neck lump)
Any dental issues or existing issues with the jaw joint (temporomandibular joint)?
Any previous ear problems or operations?
Any previous head and neck cancer?
Smoking status
Examination
Inspection of the ear, looking for cellulitis, discharge, scars.
Otoscopy: look for swelling of ear canal and exudate (otitis externa), mucopurulent discharge (AOM or COM), a red bulging TM, granulation tissue.
Facial nerve exam
Examination of TMJ (clicking, tenderness, locking, ROM)
Neck palpation
Oropharyngeal/oral examination

Normal Tympanic Membrane
Which side is this?
Differential diagnosis and primary care management
The main task is try and find out if the pain is otological in origin, or referred from elsewhere.
If the ear looks normal, the pain is coming from elsewhere.
Otological pain
Otitis externa - inflammation of the ear canal lining. Examination would reveal a red, oedematous ear canal with thick, coated exudate. The tympanic membrane may not be visible but should be normal. Give a two-week course of antibiotic-steroid eardrops (e.g. Gentisone HC or Sofradex) and water precautions. No need to swab initially. If not settling, refer to ENT emergency clinic.
For more info, please click here
Otitis Externa
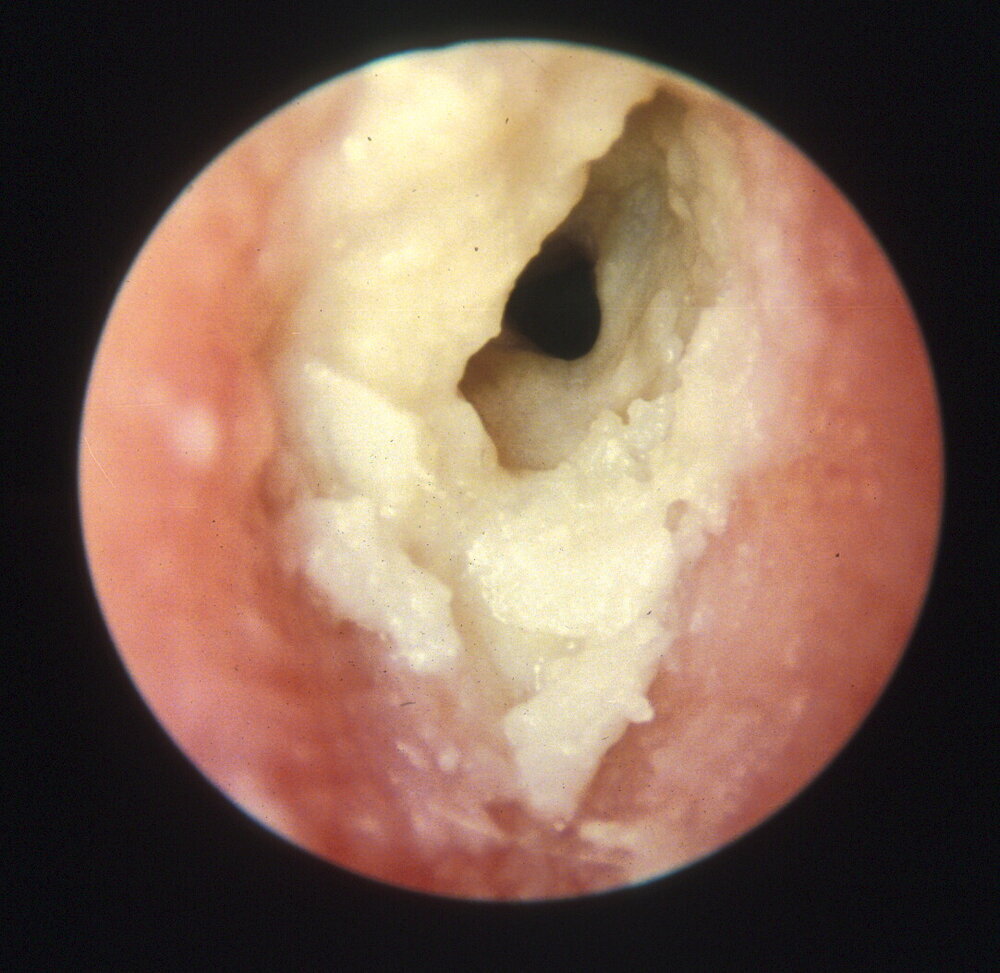
Acute otitis media - This is inflammation of the middle ear mucosa and normally presents in children. There is usually an onset of pain before the exudate appears. Examination at initial stages would reveal a bulging and red TM, which can perforate to allow the pus to discharge into the external ear. This usually results in the pain and fever resolving. Follow NICE guidance and prescribe antibiotics if patient remains unwell after an initial trial of analgesia. Some patients develop more prolonged painless discharge after AOM via the perforation - give two week of ciprofloxacin drop to prevent this becoming chronic.
For more info, please click here

Acute Otitis Media
The tympanic membrane is bulging, injected and pus is seen in the middle ear.
Perichondritis - This is inflammation and infection of the ear cartilage. Can arise from local trauma (piercing or insect bites), or progress from otitis externa. The pinna is red and swollen, but the lobule is usually spared. Mild cases can be treated with oral ciprofloxacin/levofloxacin, but if severe or worsening, refer for IV antibiotics.
For more info, please click here
Foreign body in ear canal - This is usually painless but can be painful if infected or corrosive. Usually obvious on examination. Refer urgently if patient is in significant pain. The patient should go straight to ED if the foreign body is a button battery.
For more info, please click here
Ramsay-Hunt syndrome - This is reactivation of Varicella Zoster virus (shingles) in the distribution of the facial nerve / geniculate ganglion. Patients tend to present with a lower motor neurone facial palsy and a painful ear. It is often mistaken for Bell's palsy: the differentiating factor is vesicles present in the ear canal. Treatment is high dose steroids (1 mg/kg prednisolone (60 mg max) for 1 week with PPI cover), and antivirals (e.g. aciclovir 800mg five times a day for 1 week). Adequate analgesia is also important.
Non-otological pain
Temporomandibular joint dysfunction - Causes an aching, intermittent ear pain which may be worse with chewing, talking or stress. Examination will reveal a normal ear and potentially a tender jaw joint with clicking or crepitus. It may also be tender on palpating the jaw joint from inside the ear. First-line treatment is adequate analgesia and TMJ exercises . If no better, refer for dental/OMFS input.
Musculoskeletal - spasm and tension in the spinal and neck musculature can give rise to otalgia. Examination may reveal tenderness in these muscles that would clinch the diagnosis. Treatment is centred on analgesia, relaxants (benzodiazepines) and local anaesthetic infiltration. Some practices offer acupuncture, which has some evidence.
Head and neck cancer - Patients with unexplained otalgia and a normal ENT and TMJ examination should be referred under the cancer-wait pathway. Specifically ask about red-flag symptoms: dysphagia, odynophagia, hoarseness, neck lump.
Referral pathways to ENT
Same day
Complications of acute otitis media
Complications of acute otitis externa
Button battery in ear canal
Non-resolving perichondritis
Cancer pathway
Unexplained unilateral otalgia with normal ENT, head and neck and TMJ examination
ENT emergency clinic
Acute otitis externa not responding to two weeks of antibiotic-steroid drops
Other foreign bodies in ear canal
Ramsay Hunt syndrome
Routine
Recurrent acute otitis media or acute otitis externa
Author: Mr Ananth Vijendren BM MRCS MRCS (ENT) FRCS (ORL-HNS) PhD, Consultant Otologist/ENT Surgeon, Lister Hospital, Stevenage