Hoarseness
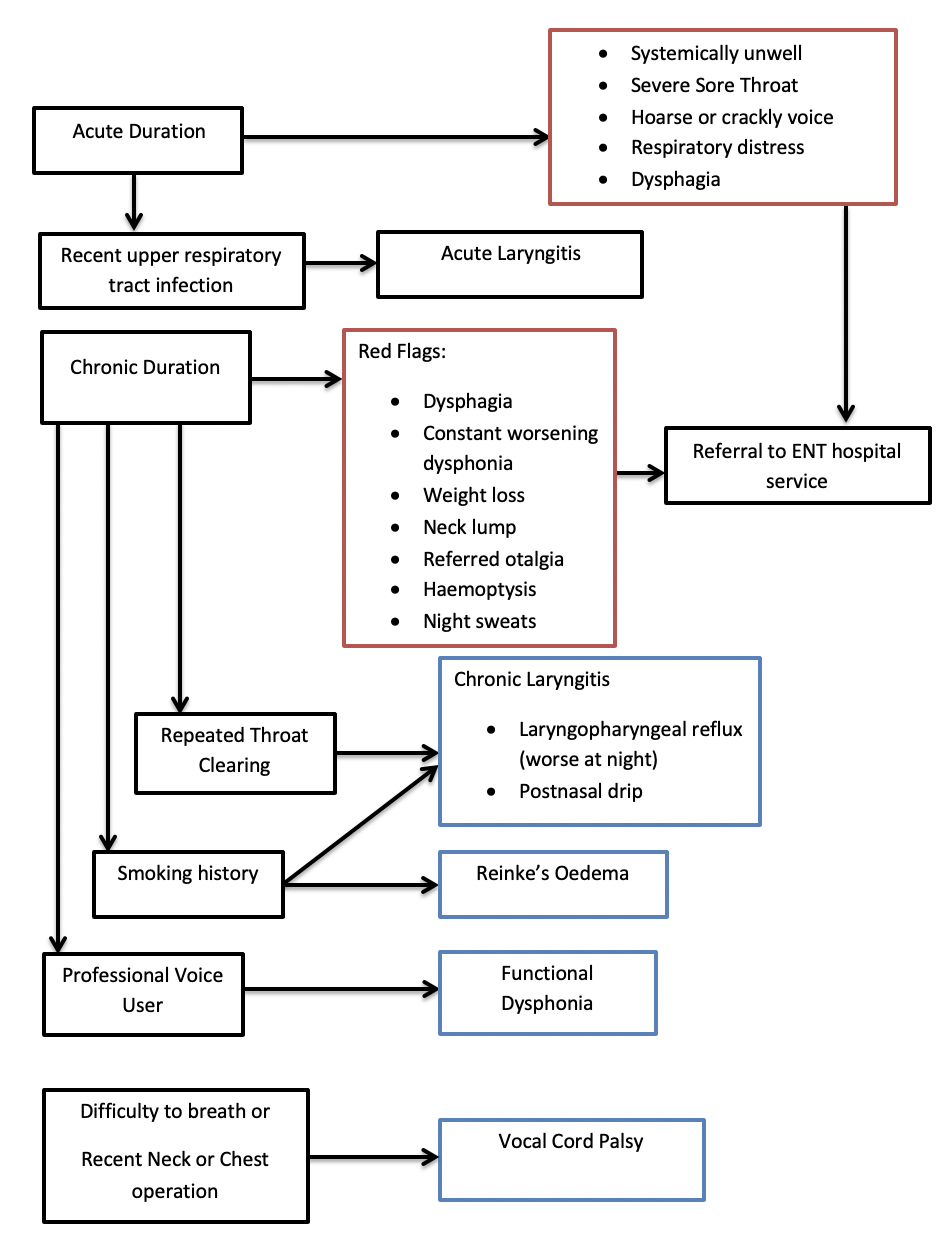
Red Flags requiring urgent ENT review
Systemically unwell
Severe sore throat out of proportion to examination findings
Dysphonia – change in voice (hoarseness or crackly)
Respiratory distress
Acute dysphagia
Assessment
History
Duration
Constant or episodic
Ability to swallow
Voice change
Voice use (profession)
Throat clearing
Neck movement and lumps
Reflux history
Previous episodes
Recent treatment or operations
Smoking history
Malignancy red flags (Weight loss, referred ear pain, neck lumps, night sweats, haemoptysis)
Examination
Mouth: mouth opening (inability to open mouth is trismus), posterior pharyngeal wall erythema
Neck: movement (inability to move neck is torticollis), lymphadenopathy or masses, skin changes
Breathing: difficulty breathing or airway sounds (stridor)
Differential Diagnosis
Epiglottitis
Acute sore throat, dysphonia, dysphagia and generally unwell. Click here for more info
Laryngitis
Inflammation of the larynx can be caused by infection (URTI), irritation (laryngopharyngeal reflux or post nasal drip), allergy and overuse/trauma (profession voice use, coughing). Laryngitis can be acute or chronic (symptoms more than 3 weeks). Patients usually have hoarseness and pain in the throat. Acute laryngitis will self resolve with voice rest, avoidance of triggers and hydration. Treatment of the cause of chronic laryngitis is vital. All patients with non-resolving chronic laryngitis should be referred to ENT to rule out laryngeal pathology.
Reinke’s oedema
Oedema of the vocal cords classically caused by smoking. It can also be caused by laryngopharyngeal reflux, hypothyroidism and voice overuse. Diagnosis is with direct visualisation of the vocal cords. Stopping smoking, reflux management and voice therapy are all management options.
Functional voice disorder
Dysphonia where there is no anatomical cause in the larynx usually occurring in voice users. Voice therapy is the management.
Laryngeal cancer
It is the second most frequent cause of head and neck cancer and 4 time more common in males. Smoking is the main risk factor. Patients who have chronic hoarseness with or without additional red flag symptoms such as: dysphagia, throat pain, neck lump, referred otalgia, haemoptysis or weight loss should be referred as a 2-week wait for review. NICE recommends all patients over 45 with persistent unexplained hoarseness to be referred as a 2-week wait. An urgent CXR is helpful to rule out chest pathology causing chronic hoarseness. Direct examination of the upper airway plus biopsy or imaging may be required.
Vocal cord nodules
Benign thickening of the vocal cord caused by overuse of the voice. Voice therapy is the most common treatment modality.
Vocal cord palsy
Patients more commonly have a unilateral vocal cord palsy which causes hoarseness, breathy voice and aspiration. Bilateral vocal cord palsy causes difficulty breathing and patients must be referred to hospital on the same day. Lesions affecting the vagus or recurrent laryngeal nerve cause vocal cord paralysis. Examples include: Lung, thyroid and laryngeal cancer and iatrogenic (post neck surgery) injury. Persistent hoarseness in patients with unilateral vocal cord palsy would necessitate a 2 week wait referral.
Referral Pathways
Same day referral
Suspicion of epiglottitis or bilateral vocal cord palsy
Cancer-wait referral
Persistent unexplained hoarseness and patients with red flag symptoms
Routine referral
Patients with episodic hoarseness not responding to conservative management
More information
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4458789/
https://radiopaedia.org/articles/vocal-cord-paralysis
Author: Elliot Heward ENT Registrar North West Deanery